

Written by: Bissan Debsi WTS-MBT World Trichology Society
Chemo-Induced Alopecia (CIA) is abnormal hair loss caused by the toxic effects of chemotherapy. The severity of ACI depends on many factors such as type of drug used, dose, duration of treatment, route of administration, as well as patient-related characteristics such as age, existence of some form of hair loss (most commonly androgenic alopecia), nutritional and hormonal status, all of which can increase risk factors for hair loss. (1)
Hair loss is considered the most distressing component of chemotherapy. Chemo-Induced Alopecia (CIA) negatively affects body image, sexuality and self-esteem such that up to 8% of patients refuse chemotherapy due to the risk of hair loss. (2) This chronic psychoemotional stress can reduce antitumor efforts and slow healing.
The most common chemotherapy agents used to fight tumors are:
- Antimicrotubule agents: A type of drug that blocks cell growth by stopping mitosis (cell division).
- Topoisomerase inhibitors: substances that block topoisomerases, enzymes that break and reattach DNA strands and are necessary for cell division and growth.
- Alkylators: substances that interfere with the cell's DNA and inhibit the growth of cancer cells.
- Antimetabolites: These affect DNA synthesis by substituting for the actual metabolites that would normally be used in DNA synthesis.
- Antimetabolites: these affect DNA synthesis by substituting for the actual metabolites that would normally be used in metabolism, for example antifolates which interfere with the utilization of folic acid.

Statistically, each chemo-therapeutic agent affects hair loss differently. Studies have shown that 80% of patients who take anti-microtubule agents will suffer from ACI. 60-100% of patients taking topoisomerase inhibitors, 60% of patients taking alkylators, and 10-50% of people taking antimetabolites will also have ACI.
The good news is that ICA is usually reversible if well cared for. As the anagen portion of the hair cycle occurs within 3-6 months , most hair regrows 3-6 months after stopping chemotherapy agents.
However, new hair growth may show changes in color and/or texture.
Permanent ACI is unusual and has only been linked to high dose chemotherapy or use of the drugs Busulfan and Cyclophosphamide, which may be the result of damage to hair follicle stem cells. (2)
Since emotional stress is the main contributing factor to ICA, it is very important that the patient consults a trichologist before starting chemotherapy, in order to identify any pre-existing hair loss condition and stabilize it beforehand.
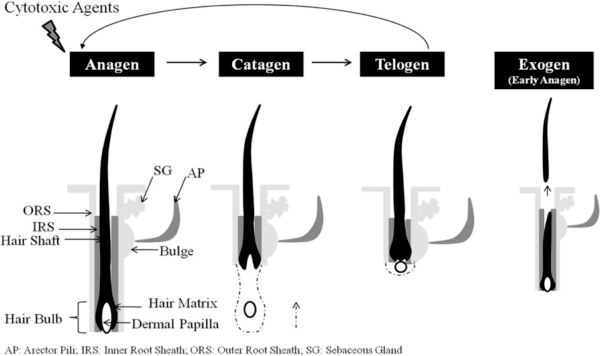
The hair follicle is a well-structured element of the skin. The papilla is a structure that forms a hair shaft moving outward from the dermis at the base of each hair follicle. It is made up of a series of rapidly dividing matrix cells. Hair development begins after birth and lasts throughout life, going through four stages, as shown in Figure 2.
As trichologists, we study the hair cycle extensively, which allows us to better understand how chemotherapy agents affect the hair.
As the catagen and telogen cycles are inactive stages, they are not affected by chemotherapy. However, when the hair is in the late anagen phase, which is marked by a lower rate of cell division (mitosis), chemotherapy accelerates the normal transition to the telogen phase.
It's easy to see why the scalp is the most affected region when you consider that up to 90% of scalp hair is naturally in the anagen phase. To learn more about hair cycles, see the following blog post: The 5 phases of hair .
When chemotherapy drugs begin, growing hair follicles develop abnormalities called hair follicle dystrophy.
- Less severe follicular damage induces the dystrophic anagen response, which occurs gradually, followed by a longer recovery phase.
- More severe follicular damage induces dystrophic catagen, which occurs immediately at the end of anagen, followed by an abnormally short telogen, and then rapid recovery. (5)
This leads us to conclude that more severe damage leads to faster recovery.
Due to ethical issues in obtaining scalp biopsies from chemotherapy patients, little is known about the mechanisms induced by chemo-therapeutic agents in human hair follicles.
Most of this important information comes from animal models of chemotherapy-induced hair loss established over the past decade.
Hair loss is a major concern during chemotherapy regimens. The development of new therapies to prevent ACI has not been studied at the microscopic level, but only from a cosmetic point of view. That is, by the degree of hair loss and the need for patients to wear headgear, such as a wig, which does not show the full extent of pathogenesis.
Therefore, various preventive measures have been proposed and attempted to minimize ACI since the 1970s, such as:
Scalp cooling has been the most widely used and studied preventative measure. Cooling agents are usually added to the scalp through a cooling cap, or the scalp itself is continuously cooled with cold air or cold liquid.
There are two scientific explanations for scalp cooling in the prevention of ICA. First, vasoconstriction, which decreases blood flow to hair follicles during concentrated administration of the chemotherapeutic agent, thereby reducing cellular uptake; and second, the reduction in biochemical activity which makes the hair follicles less susceptible to damage from the chemo-therapeutic agent.
It should be noted that some researchers have expressed concern about the possibility of scalp skin metastases (skin cancer) after cooling. However, their findings only covered a 9-month follow-up.
Scalp cooling is currently used in patients with hematological malignancies, and non-haematological malignancies undergoing chemotherapy.
There is currently no licensed therapy to treat ACI. Topical treatments intended to manage this should not interfere with the anti-cancer efficacy of chemotherapy.
Some studies show that the immune modulator AS101 (a substance that stimulates or suppresses the immune system) and the hair growth agent minoxidil are among the few agents that have been tested in humans and have been shown to minimize the severity or shorten the duration of ICA, but not prevent it.
In patients receiving a combination of carboplatin and etoposide, AS101 decreased the incidence of ICA.
For example, a 5% topical solution of minoxidil reduced the duration of ICA in breast cancer patients receiving chemotherapy and in gynecological cancer patients receiving cyclophosphamide, doxorubicin, and cisplatin as part of of clinical trials.
On the other hand, Minoxidil was not effective in preventing ACI in patients receiving doxorubicin for different types of solid tumors; and failed to induce significant hair regrowth in busulfan and cyclophosphamide-induced permanent alopecia.

Chemotherapy-induced hair loss cannot be prevented; however, it can be managed. There are currently no guidelines for pre-chemotherapy treatment. Therefore, it is crucial for a trichologist to assess the current hair and scalp condition of the cancer patient before starting any chemotherapy session.
As a trichologist, the following aspects should be addressed:
- Find out about previous or current scalp disorders (psoriasis, seborrheic dermatitis, and atopic dermatitis, to name a few), any hair loss condition prior to chemotherapy, including a family history of androgenic alopecia.
Certainly they can show a predisposition to certain forms of alopecia which can manifest themselves after chemotherapy. Obviously, the medication regimen, as discussed earlier, will be another important factor in assessing the likelihood of hair loss.
- The patient's doctor may order certain blood tests . Since any deficiency in iron, thyroid hormones and vitamin D has been linked to hair loss (6-9) it may be advisable to check blood levels before starting any form of cancer medication. (10) In addition to ANA testing to rule out autoimmune issues.
- Using trichoscopy as a tool to show the presence of early-stage androgenetic alopecia, alopecia areata incognita, or cicatricial alopecia, such as lichen planopilar or discoid lupus erythematosus, can all cause alopecia permanent even without chemotherapy and can all be made worse by anti-cancer drugs. (11-12)
- A trichogram to assess the condition of the hair before starting chemotherapy can reveal disturbances in the hair cycle, i.e. whether most of the hair is in the anagen, catagen or telogen phase, which helps predict the hair's susceptibility to adverse effects chemotherapeutic agents.
All of the trichology tests mentioned above can be used to predict the likelihood of hair loss during chemotherapy and to help control alopecia during and after treatment. Prescribing medication to prevent hair loss should be the next step. Although no drugs have been approved for ACI, some prescription or over-the-counter drugs are available.
In addition to scalp cooling, during and after chemotherapy, gentle hair care strategies, such as natural products, should be used.
To avoid further trauma, it is advisable to use a soft brush, and to wash the hair only when necessary with a mild shampoo. It is not necessary to cut or shave short hair, but it can be more comfortable. A wig can be used to help patients cope with this condition and protect the scalp from sun and cold exposure. A wig can also be used to improve the psychological deficits of patients.
The patient could also use their own hair by cutting it and implanting it on a prosthetic support. (1-4)
To prevent chemotherapy-induced alopecia, several drugs have been tried, but none have been approved. The combination of topical steroids and topical vasoconstrictors could be a useful tool to prevent massive damage to hair follicles, especially hair follicle stem cells, and thus permanent alopecia.

The best chemical treatment for accelerating regrowth after chemotherapy is topical minoxidil at a concentration of 5%. Minoxidil has been shown to increase the anagen phase and enlarge miniaturized follicles. It should be applied twice a day for at least 6 months on the affected areas. It has been shown to reduce the severity and duration of alopecia. (18-19)
Calcitriol (1,25-dihydroxyvitamin D3), which was considered the most promising agent for treating ICA, has also been used to promote hair regrowth after chemotherapy. (10).
Abbreviated version by: Jamella Bailey
You can read the original text here:
https://cruecosmetics.com/document/chemotheraoy-and-hairloss.pdf
References:
- Botchkarev VA. Molecular mechanisms of chemotherapy-induced hair loss. In:
Journal of Investigative Dermatology Symposium Proceedings. ; 2003.
doi:10.1046/j.1523-1747.2003.12175.x - Rossi A, Fortuna MC, Caro G, et al. Chemotherapy-induced alopecia management:
Clinical experience and practical advice. J Cosmet Dermatol. Published online 2017.
doi:10.1111/jocd.12308 - Macquart-Moulin G, Viens P, Genre D, et al. Concomitant chemoradiotherapy for patients with nonmetastatic breast carcinoma: Side effects, quality of life, and daily organization. Cancer.
Published online 1999.
doi:10.1002/(SICI)1097-0142(19990515)85:10<2190::AID-CNCR13>3.0.CO;2-P - Paus R, Haslam IS, Sharov AA, Botchkarev VA. Pathobiology of chemotherapy-induced hair loss. Lancet Oncol. Published online 2013. doi:10.1016/S1470-2045(12)70553-3
- Trüeb RM. Chemotherapy-Induced Alopecia. Semin Cutan Med Surg. Published online 2009. doi:10.1016/j.sder.2008.12.001
- SY P, SY N, JH K, S. C, JHL Iron plays a certain role in patterned hair loss. J Korean Med Sci. Published online 2013.
- Trüeb RM. Hormones and hair growth. Der Hautarzt. Published online 2010. doi:10.1007/s00105-009-1890-2
- REICHRATH J, SCHILLI M, KERBER A, BAHMER FA, CZARNETZKI BM, PAUS R. Hair follicle expression of 1,25‐dihydroxyvitamin D3 receptors during the murine hair cycle. Br J Dermatol. Published online 1994. doi:10.1111/j.1365-2133.1994.tb08547.x
- Aoi N, Inoue K, Chikanishi T, et al. 1α,25-Dihydroxyvitamin D 3 Modulates the Hair-Inductive Capacity of Dermal Papilla Cells: Therapeutic Potential for Hair Regeneration. Stem Cells Transl Med. Published online 2012. doi:10.5966/sctm.2012-0032
- ME L, JA K, J.S, et al. Topical calcitriol (BPM31543) for the prevention of chemotherapy-induced alopecia (CIA): Efficacy findings from a phase I safety study. J Clin Oncol. Published online 2016.
- Miteva M, Tosti A. Hair and scalp dermatoscopy. J Am Acad Dermatol. Published online 2012. doi:10.1016/j.jaad.2012.02.013
- Rudnicka L, Olszewska M, Rakowska A, Kowalska-Oledzka E, Slowinska M. Trichoscopy: A new method for diagnosing hair loss. J Drugs Dermatology. Published online 2008.
- Soref CM, Fahl WE. A new strategy to prevent chemotherapy and radiotherapy-induced alopecia using topically applied vasoconstrictor. Int J Cancer. Published online 2015. doi:10.1002/ijc.28961
- Rathman-Josserand M, Genty G, Lecardonnel J, et al. Human hair follicle stem/progenitor cells express hypoxia markers. J Invest Dermatol. Published online 2013. doi:10.1038/jid.2013.113
- Betticher DC, Delmore G, Breitenstein U, et al. Efficacy and tolerability of two scalp cooling systems for the prevention of alopecia associated with docetaxel treatment. SupportCareCancer. Published online 2013. doi:10.1007/s00520-013-1804-9
- Galimont-Collen AFS, Vos LE, Lavrijsen APM, Ouwerkerk J, Gelderblom H. Classification and management of skin, hair, nail and mucosal side-effects of epidermal growth factor receptor (EGFR) inhibitors. Eur J Cancer. Published online 2007.
doi:10.1016/j.ejca.2006.11.016 - Shin H, Jo SJ, Kim DH, Kwon O, Myung SK. Efficacy of interventions for prevention of chemotherapy-induced alopecia: A systematic review and meta-analysis. Int J
Cancer. Published online 2015. doi:10.1002/ijc.29115 - Duvic M, Lemak NA, Valero V, et al. A randomized trial of minoxidil in chemotherapy-induced alopecia. J Am Acad Dermatol. Published online 1996.
doi:10.1016/S0190-9622(96)90500-9 - Balagula Y, Rosen ST, Lacouture ME. The emergence of supportive oncodermatology: The study of dermatologic adverse events to cancer therapies. J Am
Acad Dermatol. Published online 2011. doi:10.1016/j.jaad.2010.06.051 - Wang J, Lu Z, Au JLS. Protection Against Chemotherapy-Induced Alopecia. Pharma
Res. Published online 2006. doi:10.1007/s11095-006-9105-3

